
Page 118 - Read Online
P. 118
Page 10 of 19 Kornberg et al. Hepatoma Res 2018;4:60 I http://dx.doi.org/10.20517/2394-5079.2018.86
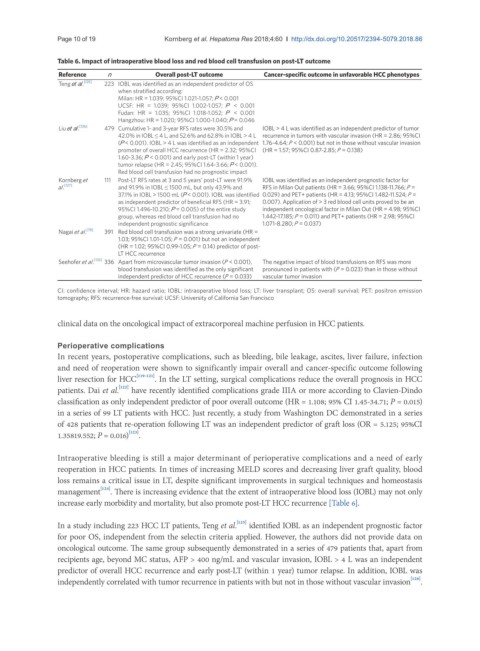
Table 6. Impact of intraoperative blood loss and red blood cell transfusion on post-LT outcome
Reference n Overall post-LT outcome Cancer-specific outcome in unfavorable HCC phenotypes
Teng et al. [125] 223 IOBL was identified as an independent predictor of OS
when stratified according:
Milan: HR = 1.039; 95%CI 1.021-1.057; P < 0.001
UCSF: HR = 1.039; 95%CI 1.002-1.057; P < 0.001
Fudan: HR = 1.035; 95%CI 1.018-1.052; P < 0.001
Hangzhou: HR = 1.020; 95%CI 1.000-1.040; P = 0.046
Liu et al. [126] 479 Cumulative 1- and 3-year RFS rates were 30.5% and IOBL > 4 L was identified as an independent predictor of tumor
42.0% in IOBL ≤ 4 L, and 52.6% and 62.8% in IOBL > 4 L recurrence in tumors with vascular invasion (HR = 2.86; 95%CI
(P < 0.001). IOBL > 4 L was identified as an independent 1.76-4.64; P < 0.001) but not in those without vascular invasion
promoter of overall HCC recurrence (HR = 2.32; 95%CI (HR = 1.57; 95%CI 0.87-2.85; P = 0.138)
1.60-3.36; P < 0.001) and early post-LT (within 1 year)
tumor relapse (HR = 2.45; 95%CI 1.64-3.66; P < 0.001).
Red blood cell transfusion had no prognostic impact
Kornberg et 111 Post-LT RFS rates at 3 and 5 years’ post-LT were 91.9% IOBL was identified as an independent prognostic factor for
al. [127] and 91.9% in IOBL ≤ 1500 mL, but only 43.9% and RFS in Milan Out patients (HR = 3.66; 95%CI 1.138-11.766; P =
37.1% in IOBL > 1500 mL (P < 0.001). IOBL was identified 0.029) and PET+ patients (HR = 4.13; 95%CI 1.482-11.524; P =
as independent predictor of beneficial RFS (HR = 3.91; 0.007). Application of > 3 red blood cell units proved to be an
95%CI 1.496-10.210; P = 0.005) of the entire study independent oncological factor in Milan Out (HR = 4.98; 95%CI
group, whereas red blood cell transfusion had no 1.442-17.185; P = 0.011) and PET+ patients (HR = 2.98; 95%CI
independent prognostic significance 1.071-8.280; P = 0.037)
Nagai et al. [78] 391 Red blood cell transfusion was a strong univariate (HR =
1.03; 95%CI 1.01-1.05; P = 0.001) but not an independent
(HR = 1.02; 95%CI 0.99-1.05; P = 0.14) predictor of post-
LT HCC recurrence
Seehofer et al. [133] 336 Apart from microvascular tumor invasion (P < 0.001), The negative impact of blood transfusions on RFS was more
blood transfusion was identified as the only significant pronounced in patients with (P = 0.023) than in those without
independent predictor of HCC recurrence (P = 0.033) vascular tumor invasion
CI: confidence interval; HR: hazard ratio; IOBL: intraoperative blood loss; LT: liver transplant; OS: overall survival; PET: positron emission
tomography; RFS: recurrence-free survival: UCSF: University of California San Francisco
clinical data on the oncological impact of extracorporeal machine perfusion in HCC patients.
Perioperative complications
In recent years, postoperative complications, such as bleeding, bile leakage, ascites, liver failure, infection
and need of reoperation were shown to significantly impair overall and cancer-specific outcome following
liver resection for HCC [119-121] . In the LT setting, surgical complications reduce the overall prognosis in HCC
[122]
patients. Dai et al. have recently identified complications grade IIIA or more according to Clavien-Dindo
classification as only independent predictor of poor overall outcome (HR = 1.108; 95% CI 1.45-34.71; P = 0.015)
in a series of 99 LT patients with HCC. Just recently, a study from Washington DC demonstrated in a series
of 428 patients that re-operation following LT was an independent predictor of graft loss (OR = 5.125; 95%CI
[123]
1.35819.552; P = 0.016) .
Intraoperative bleeding is still a major determinant of perioperative complications and a need of early
reoperation in HCC patients. In times of increasing MELD scores and decreasing liver graft quality, blood
loss remains a critical issue in LT, despite significant improvements in surgical techniques and homeostasis
[124]
management . There is increasing evidence that the extent of intraoperative blood loss (IOBL) may not only
increase early morbidity and mortality, but also promote post-LT HCC recurrence [Table 6].
[125]
In a study including 223 HCC LT patients, Teng et al. identified IOBL as an independent prognostic factor
for poor OS, independent from the selectin criteria applied. However, the authors did not provide data on
oncological outcome. The same group subsequently demonstrated in a series of 479 patients that, apart from
recipients age, beyond MC status, AFP > 400 ng/mL and vascular invasion, IOBL > 4 L was an independent
predictor of overall HCC recurrence and early post-LT (within 1 year) tumor relapse. In addition, IOBL was
[126]
independently correlated with tumor recurrence in patients with but not in those without vascular invasion .